DeKalb Surgical Associates provides answers to breast problems as well as screening and prevention issues.
If you have already been diagnosed with breast cancer or had a biopsy showing abnormal cells, see Breast Cancer.
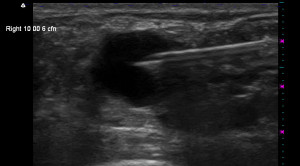
DeKalb Surgical provides answers to frequently asked questions related to benign breast problems, including breast lumps and cysts, breast tenderness and pain. Also learn about screening and prevention issues, including mammography, ultrasound, MRI and more.
Painful breast tissue is an exceedingly common symptom but is usually of “functional” origin and very rarely a symptom of breast cancer. Many years ago, a surgeon named Haagensen carefully recorded the symptoms of women presenting with breast cancer and found that only 5% of patients had pain at the time of diagnosis. And this was a long time ago when screening mammography was not used routinely; breast cancers were often much larger at diagnosis than they usually are today.
Although not typically a symptom of cancer, breast pain is a common reason for patients to seek medical attention. Breast pain appears to be aggravated by abnormal menstrual cycles and may be seen in young women with menstrual irregularity, as a premenstrual symptom, or when hormones, such as estrogen, are taken during and after the menopause. In addition, fibrocystic change, in its severest forms, may cause disabling breast pain. Although many observers find breast pain and tenderness is aggravated by excessive intake of caffeine, nicotine, or commonly used antihistamines, other investigators disagree.
Fibrocystic Change (Cystic Mastopathy, Cystic Mastitis)
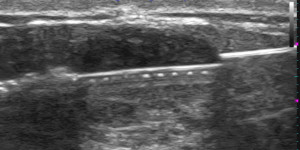
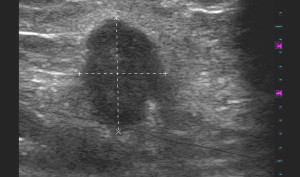
“Fibrocystic change,” popularly referred to as “fibrocystic disease,” represents a spectrum of clinical and histologic findings including cysts, nodular breast tissue, and some other changes that have technical terms like “stromal proliferation, and epithelial hyperplasia”. A fibrocystic change appears to represent an exaggerated response of breast stroma (background and supporting tissue) and epithelium (the lining of the breast ducts and lobules) to a variety of circulating and locally (in the breasts) produced hormones and growth factors. Clinically, patients with fibrocystic change have dense, firm breast tissue with lumps and frequently gross cysts or pockets of fluid. This condition is commonly painful and tender to touch. Under the microscope, the lesion recognized as fibrocystic complex contains variously sized cysts, stromal fibrosis (fibrous background tissue), adenosis (overgrowth of glands), and a variable amount of “epithelial metaplasia and hyperplasia”. All these changes can occur alone or in combination and to a variable degree in the normal female breast. Autopsy studies have questioned whether any of these changes, except perhaps macrocysts, are abnormal. In fact, all of these lesions occur commonly in the breasts of elderly patients and appear to have no particular tendency toward evolving into breast cancer. Since these sorts of changes are so common, it really is not appropriate to term it a “disease”. Nevertheless, the term “fibrocystic disease” is so commonly used, it would be hard to get everyone to stop using it. But ideally, the term fibrocystic disease should be abandoned in the absence of any well-defined clinical and pathologic syndrome.
There is no consistent association between fibrocystic changes and breast cancer. It is well established that women who have undergone breast biopsy for any reason, regardless of the underlying pathology, have a slightly higher risk of developing subsequent breast cancer. Moreover, the incidence of finding fibrocystic disease in autopsied breasts from women dying of causes other than breast cancer exceeds the incidence of these same changes in cancer-containing breasts. For those patients with fibrocystic changes, the higher risk appears to concentrate in those whose biopsy specimens show abnormal ductal and lobular hyperplasia and, to a lesser extent, cyst formation. Therefore, the fibrocystic complex appears to be an exaggerated or abnormal response to otherwise physiologic stimuli in most patients and represents a health risk only in certain subsets.
Mammography is not a perfect screening test, and an understanding of its benefits and harms is incomplete.
Benefits
Harms
Making a Decision
There is an online tool from the National Cancer Institute which you may use to determine with some precision what your personal risk of developing breast cancer is. It’s called the Breast Cancer Risk Assessment Tool.
Here’s a useful decision aid available through the University of Sydney in Australia. It takes about 30 minutes to go through the steps. In the end, it gives you the option of documenting your own personal decision aid.